
Description
The UMKC-IHD and the Kansas University Center on Developmental Disabilities (KUCDD) are partnering on a Field Initiated Program grant from the National Institute on Disability and Rehabilitation Research (NIDRR) with the goal of testing the Self-Determined Career Development Model (SDCDM) with a multi-state sample in Missouri, Kansas, and Oklahoma to measure the gain individuals with DD make in self-identified career development goals as a result of their interaction with the model.
- Project Contact – George S. Gotto, 816-235-5334 and Megan Steele, 816-235-6438
- Project Period – 2012 – 2015
- Project Funding – $200,000 (FY2014)
- Funding Source – National Institute on Disability and Rehabilitation Research
Core Functions
Applied Research
Data collection, entry, and analysis occurs under the direction of the UMKC-IHD faculty.
Community Services and Supports
Institute faculty provide all training and technical assistance to the community partners who are participating in project activities.
Information Dissemination
IHD faculty have developed all training and facilitation materials that are being used to implement the SDCDM.
Program Need and Historical Context
Employment figures for adults with I/DD lag far behind those for the general population; the Alliance for Full Participation reports an employment gap of 58% between people with I/DD and the general population (2009). People with I/DD who are working tend to work fewer hours and make less per hour than their counterparts in the general population, and tend to be concentrated in low-paying entry-level service jobs (Butterworth, et. al., 2011). In Missouri, according to 2009 data from the Institute for Community Inclusion (ICI), just 7% of individuals with DD/ID were employed in integrated settings, compared with 20% nationally.
Consumer and Community Involvement
The DDHI includes a Community of Practice (CoP) made up of 20 direct support organizations, parks and recreation organizations, and university partners. The purpose of the CoP is to create and test advocacy strategies that support implementation of the recommended policies and practices within these organizations. The diversity of viewpoints is a strength the group can use to forge new collaborations and find innovative solutions. The DDHI CoP will include a range of perspectives and models for supporting people with DD to make sustainable healthy lifestyle changes and choices.
Significant Project Activities and Outcomes
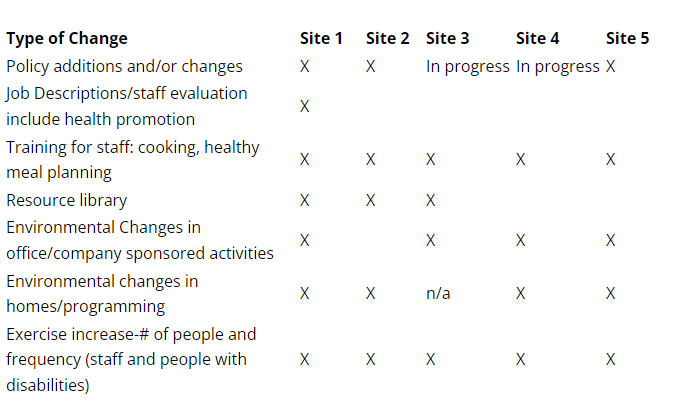
To date a total of 49 people who work at organizations that are participating in the DDHI have completed the Health Matters Assessment of Needs. The majority of these people (34, 70%) are from organizations that did not participate in the DDHI in Year 1. Preliminary results from the data show that those organizations that have participated in Years 1 and 2 are much more likely to offer health programs (13, 87%) than the organizations that have only participated in Year 2 (4, 12%). Those organizations that have participated in both years of the DDHI are also much more likely to have a wellness committee (11, 73%) than the organizations that began participating in Year 2 (1, 2.9%). Finally, the data demonstrate that the organizations that have participated in Years 1 and 2 of the DDHI are more likely to promote healthy eating (13, 86.7%) and exercise (10, 66.7%) using messaging in their building. The organizations that have only participated in Year 2 lack messaging that promotes healthy eating (5, 14.7%) and exercise (12, 35.3%). Five model sites from Year 1 made at least three changes in policy and practices after using the Policy and Practice Review Tool that was developed in that Year. Five out the six model sites made (or are in progress and waiting for approval) policy changes/additions to expect healthy practices of staff in their work supporting people with disabilities.
Institute’s Role
- Co-facilitate strategic planning activities with participating organizations
- Lead needs assessment and evaluation activities
- Serve as Liaison to community public health and recreation work group
- Provide technical assistance and support the development of training and products
Products
The Healthy Lifestyles Policy and Practice Review (HLPPR) Tool will help community living support organizations to revise policies and practices that impact: (a) social supports that promote healthy lifestyles (i.e., available for clients and employees, promotional messages, wellness committee); (b) physical activity of clients and employees; and (c) healthy food choices of clients and employees.
